Coronavirus: How to Do Testing and Contact Tracing
Part 3 of Coronavirus: Learning How to Dance
Our previous articles, Coronavirus: Why You Must Act Now, The Hammer and the Dance, and Out of Many, One have gathered over 60 million views together and have been translated into over 40 languages. This installment is part 3 (part 1 and part 2) of our 4th article, Learning How to Dance, a series that focuses on the specific steps required to open up the economy. Translations in 12 languages below, more welcome. To receive the next installments and articles, sign up here.
Summary
We can reopen the economy again if we do a few things right, including testing and contact tracing. We need to test all people with symptoms and their contacts, which means at most 3% of our tests should turn out positive. We need to identify as many infected as possible, and 70% to 90% of their contacts, to isolate or quarantine them. If we do all of that really fast (within a day or so), it might be enough to control the epidemic. We should hire lots of people to do that, and also use technology. The technology has some privacy tradeoffs, but they are really reasonable. Most of the bluetooth contact tracing apps built today are amazing pieces of technology that will be useless unless they get some fundamental changes.
Many countries are enduring the Hammer today: a heavy set of social distancing measures that have stopped the economy. Millions have lost their jobs, their income, their savings, their businesses, their freedom. The economic cost is brutal. Countries are desperate to know what they need to do to open up the economy again.
Thankfully, a set of four measures can dramatically reduce the epidemic. They are dirt cheap compared to closing the economy. If many countries are enduring the Hammer today, these measures are the scalpel, carefully extracting the infected rather than hitting everybody at once.
These four measures need each other. They don’t work without one another:
- With testing, we find out who is infected
- With isolations, we prevent them from infecting others
- With contact tracing, we figure out the people with whom they’ve been in contact
- With quarantines, we prevent these contacts from infecting others
Testing and contact tracing are the intelligence, while isolations and quarantines are the action. We’ll dive into the first two today — testing and contact tracing — and the next two will be covered next.
Testing
Testing has been at the core of the conversation for weeks. In most countries, people criticize the lack of testing. But few people ask the question: How much testing should we have?
How Much Testing Do Countries Need?
That depends on the country and what it’s trying to do. There are two types of countries.
On one side, we have countries like the US, Spain, UK, or France that have an epidemic that is out of control. They weren’t prepared to handle the crisis, so they applied the Hammer, a series of very heavy measures to lock down the economy and prevent people from getting infected. This is how they stop the epidemic. For them, testing massive amounts of people is not necessary at this point, because they limit the spread with the Hammer. The only people they need to test are those who are sick or likely to get sick (eg, healthcare workers), to isolate them and treat them. Most of these countries are the ones in red or orange here.
But before the countries in orange or red go into the Dance, they will need to be ready. That means massively ramping up testing to get closer to the second type of countries, in green.
These include the likes of Taiwan, Vietnam or South Korea. They also use tests to diagnose patients, but they have another use too. They trace the contacts of the infected and test them, even if they don’t have symptoms. They also broadly test anybody else who might be infected but doesn’t know it yet.
To test the additional groups of travelers or contacts traced, you need much more testing than to just test people with symptoms. That’s why only approximately 1%-3% of their tests find somebody infected. All the developed countries that have controlled the epidemic have that level of positives.

For most developed countries, the worse their testing has been, the worse their epidemic. The group of countries circled in red has had few tests and devastating outbreaks, while the countries at the bottom left had great testing and few cases. When the countries that are managing the crisis the best are doing a lot of testing, other countries should follow their lead, which seems to be around 3% of positives.
Singapore and Germany are interesting cases. They used to have ~3% of positives, but with the recent outbreak, they went up to 8%. Hopefully, this is not a problem of capacity and they can test everybody they want; they are just finding many more positives. But it might show how an outbreak can overwhelm testing capacity, making it harder to identify all cases and isolate them, and making it harder to stop it.
Governments want to predict when they will have enough testing, but that’s hard because both their number of tests and cases are constantly changing — and in fact cases are also influenced by testing, since more testing will find more cases. So how can they predict when they’ll be testing enough?
In this graph, daily new cases are the red line and daily new tests are the green line. They have been scaled, so that they can be compared. As we just saw above, the experience of countries that controlled the epidemic indicates we should aim for at least 3% of positives, which means you want ~33 times more tests than cases. So the tests axis on the right is ~33x bigger than the cases axis on the left. With that you can easily see when you have enough tests.
In South Korea, when the outbreak really picked up, suddenly the number of cases was too much for the number of tests, and they lost confidence in the official numbers of cases (red area). However, within weeks, they were able to have enough tests to get into the green zone again. Now, every day, they are making many more tests than they need to be above the 3% threshold. It is around 1%.
Compare that with Italy.
As you can see, Italy has been consistently ramping up their number of daily tests, but they’re still not enough to know the extent of the situation. However, with this graph, they can start having a sense of when they will cross that threshold. If cases keep going down while tests keep going up, they might cross in a few weeks.
Here are a few more countries:
These graphs clearly show how far away most countries are from testing enough.
With enough testing, you can enter the Dance phase. You can manage the epidemic by isolating cases and quarantining their contacts. By doing this, you can quickly identify those who are contagious or likely to be and then prevent them from infecting others, and as a result, you can protect your population without having to lockdown everyone and limit their freedom. People can go out, and you can reboot the economy. That’s why it’s so important to test more, and to increase testing until only 3% of people test positive.
If they don’t test enough, they don’t isolate the infected, so they don’t know where they are, and they’re forced to apply a lockdown.
As long as testing is limited, countries must also decide who they test first. How can they prioritize the few tests they have?
Priorities for Testing
As we said before, the first people you test are those with symptoms, usually at the hospital or the doctor’s office, to know who to treat and isolate. This is most of what countries do during the Hammer.
For countries getting ready to dance, once they’ve covered the symptomatics, they need to start testing those who don’t have symptoms yet. That’s what contact tracing allows: finding out who might be sick, and testing them.
If you read our previous post, you have seen this graph:
As a reminder, it comes from a great paper from Oxford University published in Science. It goes through great lengths to identify how the coronavirus spreads from person to person. The horizontal axis shows days since the first infection, and the vertical axis shows how many other people are infected in different ways on any given day. For example, on Day 5 after contagion, carriers infect on average close to 0.4 other people. Most of that comes directly from people who are already symptomatic or who will soon become so (so they’re called pre-symptomatic). A little bit of it is through the environment (probably surfaces), and even less comes from people who have the virus but will never develop symptoms.
Testing and contact tracing are the intelligence; isolation and quarantines are the action.
If you only test and isolate people with symptoms, you can reduce R (the effective transmission rate) by 40% at most. If R is 2.5 or 3, as in the current epidemic, that won’t get you below 1.
But if you also trace their contacts and test them, you can now also catch the pre-symptomatics, reducing contagions up to 85%.
In summary, you need a lot of testing for both those with symptoms and all of their contacts.
But that can only get you an 85% reduction in R if your testing is perfect. In real life, it takes some time. How much does that matter?
The Importance of Speed in Testing
If your testing operation isn’t quick enough, or if it’s too hard or expensive to get tested, people won’t get tested on time or the results won’t be quick enough. As a result, a share of the infections will have happened before you have time to isolate these cases.
The same concept is true for contacts traced. If you take on average three days from infection to track contacts and quarantine or isolate them, you will miss a lot of contagions.
We’re seeing three factors that matter here:
- How many infected we identify and isolate
- How many contacts we trace and quarantine
- How quickly we do both
How can we compare the importance of these three factors? Let’s imagine first we have immediate testing and contact tracing.
This graph, extracted from the Oxford paper, tells you how many infected people and their contacts you need to identify, so you can isolate or quarantine them and reduce the transmission rate of the epidemic.
The epidemic grows in the red/orange zone, and shrinks in the green zone. The limit is the black line, with the dotted lines as the confidence interval (representing uncertainty). Any point on that line is supposed to be enough to control the epidemic. So, for example, if you note the position of the red X, it shows you could control the epidemic if you could instantaneously isolate 60% of patients with symptoms before they infect anybody else, instantaneously trace over 50% of their contacts, and isolate/quarantine them before they infect anybody.
That sounds hard. The good news is that, done well, this measure alone could stop the epidemic. But even if you don’t do it well, it contributes. For example, isolating 50% of infected and 30% of their contacts will get you closer to the green area. That’s good. Combine this with other measures such as mask wearing, and you’re getting closer to epidemic control, without the need of a Hammer.
The other thing that this graph assumes is no delay between the infection and testing or contact tracing. But delays are inevitable in the real world. How much do they matter?
The graph from the right is the same one shown above. The three other graphs show what happens if there is a delay of one day, two days, or three days in isolating symptomatic and asymptomatic people.
Let’s look at the graph all the way to the left. It’s basically telling us: “If you have a 3-day delay in isolating and quarantining cases, it will be awfully hard to stop the disease.” Every bit contributes, but with this type of delay, it contributes very little.
The second graph tells us: “If you have a delay of just two days in both isolating and quarantining, you need to be able to isolate at least 70%-90% of infected, and trace at least 70%-90% of their contacts to stop the epidemic just with this measure.”
Put another way: you can control the epidemic without shutting down the economy and just with this single group of measures if you’re fast and effective at testing people, isolating the sick, tracking their contacts, and quarantining them. You need to do that super fast and really effectively, or else you won’t be able to control the epidemic just with this measure.
Without executing this set of measures well, it will be awfully hard to control the epidemic, and you’ll be forced to either find some other miraculous set of measures, go for herd immunity, or apply another Hammer — with all their economic costs or massive deaths.
This is why it’s so important for countries to have lots of testing that works as fast as possible. You need both: the quantity and the speed.
South Korea’s drive-through testing and phone booth testing offer a model. The easier it is for people to get tested, the more people will do it quickly, and the better we will control the epidemic.
Some countries are considering testing everybody all the time. Imagine, for example, that most of the population of the US was tested every week — say 300 million of the 330 million. That would tell the country everybody who is getting sick at any time, and likely control their epidemic. Doing 300 million tests every week is a bit far off now, however, and might be a bit expensive. In a year, that’s over 15 billion tests. If we assume they’re very cheap because of the volume — let’s say $20 each — that’s $300 billion, which is quite expensive, even if just 15% of the $2 trillion stimulus.
This is extremely expensive and not realistic today. But if we could have efficient ways to test more people, the calculation could change.
There are ways. For example, this paper explains how, if few people are infected (i.e., if your prevalence is low), you can cleverly test a bunch of people at once and reduce the number of tests needed eightfold. Dropping the cost of mass testing from $300 billion to less than $40 billion would be a huge improvement. Many countries are already doing it, such as Germany, Austria, Israel or the US.
Another very promising approach is sewage testing.
The idea is that we can measure how much coronavirus there is in sewage, which can tell us broadly how many people are infected. From there, we can test sewage upstream to find the buildings where the virus comes from, test everybody in that building, and isolate the infected.
In summary:
- You need to test a lot, to identify infected people as soon as possible.
- That means enough testing so that only 3% of your people tested turn out positive, since that’s what successful countries are seeing.
- You also need to test very fast, so you can isolate the infected immediately and reduce how many other people they infect.
- That is half of the battle. The other half is testing all contacts to identify who else is infected but has not developed symptoms yet. 45% of infections come from them.
- Similarly, you want to do that contact tracing very fast, to reduce the period of pre-symptomatic infectiousness.
- There are ways to do testing efficiently, testing several people with one single test.
- There are other promising approaches to testing, such as sewage testing.
- In a perfect world, we can test everybody all the time. We might get there, but in the meantime, it looks expensive and hard.
- So in the meantime you need to prioritize who you test. First, people with symptoms. Then, all their contacts.
That leads us to contact tracing.
Note: We will cover serological tests and other testing details another time.
This section draws heavily on ideas and sources from @Genevieve Gee’s research on Testing. Notably, the idea of tracking % of positives is hers.
Contact Tracing
This is by far the meatiest section in the entire article. That’s intentional: The stakes are extremely high. As we just saw, not only can good contact tracing slash transmissions; it’s vital to moving from the Hammer to the Dance, to reopen an economy safely. But it’s also very complex and poses many privacy questions.
But before we dive into it, we need to get a good sense of what exactly it means to trace contacts.
Let’s call Bob the person who has been infected. We want to identify as many of his contacts as possible, as fast as possible. The ones that matter are not all people he’s met, but rather the ones that might have been infected.
To do that, you need a team of contact tracers.
Contact tracers have several functions. First, they are given a list of people like Bob who have been infected. They interview Bob to learn everywhere he’s gone over the last couple of weeks and who he’s been with. Since Bob is human, he’s frequently unreliable: He might be forgetful, sick, panicking, sad, uncooperative, or all of the above. So contact tracers also use technology to help. An example might be South Korea, where tracers use mobile GPS data, credit card spending data, and CCTV footage. Another example might be using results from a contact tracing app.
With all that information, they put together a list of Bob’s contacts who might have been infected, ordered by likelihood of infection. Then, they call all these contacts. Depending on the likelihood of infection and the government’s rules, they might order them to get tested, self-quarantine, or just check on their symptoms. They want to catch as many contacts as possible, as fast as possible.
But what qualifies as a contact? How many contacts do we need to trace? How fast do we need to trace them?
What Qualifies as a Contact?
Since most people are believed to be infectious for around two weeks only, we only care about people that Bob might have been in contact with over the past couple of weeks. Before that, Bob was unlikely to be infected, and if he was, his contacts are unlikely to be infectious anymore.
Within these two weeks, we only want to identify those likely to be infected. Bob’s family members are all very likely. Conversely, you don’t care as much about the people he crossed on the street 5m away (~15ft).
As we saw in The Basic Dance Steps Everybody Can Follow, contagions are much more likely to happen in confined environments where people are close to one another, speaking, coughing or singing for a long period of time.
Countries convert that into rules. For example, they investigate Bob’s contacts if they spend over 15 minutes together within 2 meters. That sounds reasonable. But in reality, tracers are much more subtle than that. A person that shared a meal for one hour sitting face to face might be marked as high risk and asked to go on quarantine, with investigators checking in every few hours, while a person that shared the line at the grocery store might be asked to just be extra careful and check her symptoms frequently.
How Many Contacts Do We Need to Trace?
We saw before that we wanted to trace at least 60% of contacts and quarantine/isolate them immediately to substantially reduce R (the effective reproduction number, how many infections are caused by a carrier of the coronavirus). But that paper assumed a certain R0 of 2.5 (R0 is the reproduction number in perfect conditions: when nobody is immune yet, and no measures have been taken against it). What if it’s different?
This paper looks at that. It takes different R0s and assesses what share of contacts we need to trace to bring R down below 1. Each line below represents a different R0 of 1.5 (red line), 2.5 (grey line) and 3.5 (brown line).
The horizontal axis tells you the share of contacts traced, and the vertical axis the impact on R.
Let’s take the brown line at the top, with R0=3.5. If you don’t do anything, you have a transmission rate of close to 3: Every person infects 3 other people (it’s not 3.5 because the paper assumes some isolation of infected patients). Then R goes down as more and more contacts are traced and quarantined.
You can see that the brown line goes below the dotted line of “1” at around 90% of contacts traced. That means that you need to trace 90% of contacts — and make sure they don’t become infectious — to stop the epidemic. If you do that well, this measure alone can stop it. But thankfully, even if you don’t do it perfectly, it still helps.
You can see that the brown line has some area around it. It shows that these calculations are not perfect yet. We’re lacking a lot of data, so we need to make some guesses. It might be that tracing 90% of contacts only gets you to R=1.5, or to 0.5. We’re not sure. But it definitely lowers it substantially.
If instead of R0=3.5, we look at R0=2.5 (the grey line), our best guess is that identifying 70% of contacts is enough to stop the epidemic.
Let’s keep these numbers in mind: Based on all our data, we want to trace between 70% and 90% of contacts, as fast as possible, to have as big an impact as we can reducing the epidemic.
According to one paper, that translates into around 20 to 30 contacts to trace per infected.
How Many Investigators Do You Need?
This is how Johns Hopkins is thinking about it:
According to this Johns Hopkins plan, the US would need 100,000 contact tracers. Other calculations put that number at 300,000. That’s a very wide range. It reflects the very wide range of this graph, which shows a 10x difference between Wuhan and New Zealand. Why?
This gap in the number of contact tracers needed per person doesn’t make sense. If a country has 1 million people and zero infections, and another country also has 1 million people but 10,000 infections: Should they have the same number of contact tracers? No. The population is meaningless.
When you’re hiring contact tracers, you’re buying their time. The time needed depends on the number of cases and the time per case.
The number of cases is different per country and depends on how the epidemic is going. The time needed per case depends on training and technology. Let’s take a couple of examples to get orders of magnitude.
At its peak, Hubei had 1,800 teams of 5 investigators doing contact tracing. That’s 9,000 investigators. The peak number of official cases was around 4,000 cases. Let’s assume that the 9,000 investigators were hired on average a few days after Hubei was locked down, and were able to clear the backlog of cases around a month later, when the crisis subsided.
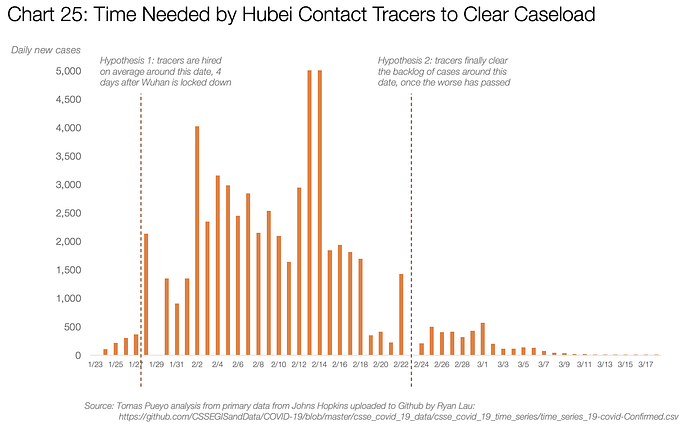
Between these two dates, 9,000 tracers working for 27 days (assuming no weekends) would have been able to process around 63,000 cases, which means around 4 person.days per case (a person.day is one person working for a day. So 4 person.days can be 4 people working on something for a day, or one person working on it for 4 days, for example). If we assume they were hired a few days earlier and cleared cases later, it might get that number to 5 or 6 person.days per case, not much more.
Contrast this with a former head of the Centers for Medicare and Medicaid Services:
According to this, the cost of a case is 12–15 person.days.
Let’s assume a country has 10,000 new cases per day — and it’s confident this is the case because its testing is giving around 3% of positives (as we saw in the testing section, this is a good number to get a good sense of what is truly happening).
Let’s assume they have no contact tracing technology, so investigators need to call the infected people, interview them, and then call all their contacts and interview them one by one. Each one of these conversations is very long, because people don’t remember with whom they ate lunch two days ago, forget about two weeks ago. Then they need to file reports, analyze the data, cross-reference it across cases…
If it takes them 15 person.days per case, we will need 15*10,000=150,000 person.days of work every day — so we need to hire 150,000 people. If you need to cover for weekends, holidays, sick days, etc, you might get that number to 200,000 or so. Assuming $20 per hour all costs included, that’s $7 billion per year. That is reasonably expensive, but a drop in the bucket compared to the cost of the current economy shutdown.
Imagine instead that we have just 1,000 new cases per day instead of 10,000. Our need drops to 20,000 workers per day.
Unfortunately, both of these scenarios take three days, since they both require five people working on a case for three days. Yet as we saw, time is critical.
Imagine now that we still have 1,000 new cases per day, but our contact tracers are as productive as those in Wuhan, where a team of 5 can clear one full case per day. With 5,000 contact tracers (~7,000 including holidays etc), you can cover all the cases within one day instead of within 3.
These numbers are just approximations. The goal is to highlight how to think about this, to encourage countries to quantify and minimize that cost, and give broad orders of magnitude. These orders of magnitude help us realize many things:
- It’s very hard to rely on contact tracing while an epidemic is raging. With the ~30,000 new cases per day that the US has at the end of April, if they need 15 person.days per case, they need to hire over 500,000 people to do this well. It’s very hard to do that quickly and effectively. One of the values of the Hammer is to bring that number down, so that it’s manageable for contact tracers.
- It also illustrates that, if a country has another outbreak, like in Singapore or South Korea, local Hammers might be necessary, since those outbreaks overwhelm the capacity of contact tracers.
- If a team of 5 tracers really takes 3 days to fully process a case, that is just too slow. A lot of the contagions will have already happened.
- It’s also likely that these people, manually, can’t catch all the contacts they need to catch. The manual process of the Anchorage contact tracing team from the picture might be a pioneer in the US that is enough for Alaska, but it doesn’t scale for most states or countries. It needs to be much more effective.
Let’s imagine that Bob (red dot, infected) is pretty social and has had significant interactions with 55 contacts over the last two weeks. In a conversation with a contact tracer, it might be easy for him to tell her about his four family members. After going through his calendar, he might be able to tell her about eight co-workers with whom he’s had meetings. He remembers he had dinner with four more friends, and a trip he made to the grocery store.
After looking at CCTVs, the tracers can see Bob’s movements at the grocery store and identify two more contacts to trace, for a total of 18 contacts. Since the tracers don’t have the phone numbers of the work contacts or the identity of the people at the grocery store, they now need to talk with the employer and store to get these contacts. That’s assuming Bob is cooperating.
18 cases is less than half, and unfortunately it took 3 days to investigate them. Remember, ideally we need 70% to 90% within one day. But with this process, we are relying on Bob’s cooperation and memory, as well as going through hoops to get all the data. That’s just not enough.
A country that has done this really well is South Korea. How do they do it?
Technology for Contact Tracers: Personal Data from the Infected
South Korean contact tracers have access to the GPS and credit card spending data of those infected like Bob. Thanks to them, it is quite easy to figure out where Bob has been over the last 2 weeks (green squares on the chart).
With Bob’s memory refreshed, it’s much easier to identify all the people he might have met. And that can be complemented now with CCTV and other things, like access to the bus or gym tagging systems. As a result, in this hypothetical scenario, we go from 18 to 41 contacts traced. It’s not yet 55, but it’s much closer to that. It’s already 75%, which would put us in the range of what has a dramatic impact on the transmission rate.
These numbers are approximations, but they reflect the reality of South Korea. This is how they’re doing it, and they’ve avoided all new outbreaks. This signals that doing this well might be enough to control the epidemic, without anything else.
There’s another huge benefit to this that we haven’t discussed yet.
In our article Coronavirus: Learning How to Dance, we explained how South Korea published where infected patients had been and at what time. People can quickly see if a place where they’ve been had an infection, to know whether they might have been infected themselves, and go get tested.
Additionally, people can download this information to their phone and use apps that automatically match the official data about infectious places with their own mobility data. That way, if you have one of these apps, you can immediately know if you came across somebody infected.
Because there’s an immediate benefit to you (“Oh there’s an app where I can see if I’ve been somewhere infected? I wanna know!”), people are likely to download such an app and use it.
For all of the above to be possible, the authorities need to have access to credit card spending and phone mobility data for infected people like Bob.
That means it’s time to talk about privacy.
The Privacy of Contact Tracing
Note: We have talked with several epidemiology and privacy experts to create this section, but our conclusions are not final. We put forward the thoughts below to further the debate around contact tracing and privacy, and invite other experts to debate these ideas with us.
Some people might read this and have an immediate reaction that it’s not acceptable because it violates people’s privacy rights, pushing the government towards a slippery slope of data gathering and privacy violations like the one the US still suffers from the 2001 Patriot Act.
That is a debate we’ll get into later, but it’s completely irrelevant at this point: Critics don’t realize that in many countries, laws don’t really need to change to achieve what’s above, because of something that’s called a notifiable disease.
The Privacy of a Notifiable Disease
Bob is infected. Because of that, he is a health hazard to the community. That means he has different privacy rights, and has had them for centuries in many countries, such as the UK or France. Many more countries, like Australia, have similar rules. In the US, they’re at the state level.
It makes sense. We’ve forgotten how devastating infectious diseases can be.
In this graph, we can see how death rates swung massively from one year to another due to epidemics in the US. But as measures were implemented, such as clean water of chlorination of water, all spikes disappeared.
This is what an unbridled epidemic looks like. At that time, it was common knowledge that the sick did not have the same rights as the healthy, because they were an existential threat to society. Identifying them and isolating was crucial, so authorities had the right to do it.
This is still true today for long lists of diseases. But the concept is the same: If you are a threat to society, authorities should be equipped to remove that risk.
If the coronavirus was labeled as a notifiable disease, doctors would have to immediately report positives to the authorities. These should then be equipped to use the resources, data and tools they already have to trace Bob’s contacts.
These three steps (having a disease in the list of notifiable diseases, a process to notify the disease to the authorities, and the privacy rights waived in these cases) usually correspond to three different pieces of legislation in every country, so they all have different takes on what to do.
But for the countries that send Bob’s file to the authorities, this is no different from the police getting access to mobile phone or credit card data from a bad actor, to identify and locate him. They can already do it, and they should be able to do it here without granting special powers that go down any slippery slope.
Whether there is a tech solution to have easy access to GPS and credit card data or not, it doesn’t matter: Contact tracers should already have access to this type of information. Making it artificially hard for them is nonsense.
As far as we could tell, this is the level of privacy that South Korea has, so it might be enough to solve the problem. They approved special legislation for this after the MERS outbreak in 2015, so other countries can do the same.
Let’s say it again: This is an invaluable tool to properly stop the massive outbreaks we’ve had around the world, and it doesn’t require a massive privacy debate. We should focus our attention on getting this done.
But we can do more. The real privacy debate should be about that: Should the authorities also have access to data from people who are not officially infected yet?
The Privacy of Contacts Traced
Now imagine that, on top of the credit card and mobility data from Bob, our contact tracer received a list of potential contacts from mobile operators.
Mobile operators know your position at any time. They could record this, along with other people who are close to you, and whenever two people are close to each other for a period of time such as 2m (6ft) for over 10 minutes, they record a match. Countries that only have one main mobile operator can do that easily, but countries with more operators could also create such a database together, in a way that prevents each company to see the data from other companies’ customers.
The government can send a request to get all of Bob’s contacts and where and when the contact happened, without knowing any further detail about the rest of the population.
There would be many false positives — for example, GPS can tell height, but it’s possible the data is thrown out in some step of the process. As a result, today, in an apartment complex, it would look like all the people living in the apartments that belong to the same vertical are your contacts. But a contact tracer can exclude most of these by eliminating all the matches that happen consistently at home and don’t live with you.
The data given to the government in this situation is exactly the data we want the government to have: just the personal mobility data from the infected on one side, and the matches with contacts on the other side. Nobody has a lot of data on people’s movements that they didn’t use to have, except for what’s critical to have for this specific situation.
Mobile operators also don’t have access to more data than what they usually get. This preserves privacy while enhancing contact tracing.
The downside of this is that GPS is not precise enough, and there might be some contacts missed and some other contacts added that shouldn’t have been. GPS can actually be made more precise if the US military decides to give access to the more detailed version it has, but it might not want to — or with AI tools. But it might be that the precision is so bad that this solution is utterly useless. Maybe it only works in low-density areas. I have not yet seen an analysis that studies this in depth. I look forward to them.
This limitation is why so many countries have joined the bluetooth app craze.
What It Would Take for Bluetooth Apps to Be Useful for Contact Tracing
Let’s assume now that our contact tracers have access to Bob’s data, and on top of that they can rely on contact data from bluetooth apps available in the market.
If you’re not acquainted with these bluetooth apps, the way most of them are conceived is that people download them and set them up so that, when they’re open, they register anonymous codes of all the people they get close to — as long as these people also have a similar app enabled. This is what Apple and Google have agreed to enable.
If Bob has one of these apps, he can notify that he has been infected by the coronavirus, and that he wants to send this information to the authorities.
So how many people would want to use such an app?
If you read our first installment, you know that Singapore’s official bluetooth app, TraceTogether, has only 20% penetration. Iceland, another country that should be able to achieve high levels of adoption, claims just 40% penetration. India released an app downloaded by 50 million people, which sounds like a success until you realize it’s less than 4% of the population.
Let’s be wildly optimistic and assume that most countries can do 50% better than Singapore — unlikely, since it is very rich, everybody has a smartphone, education is very high, and people trust the government — and get 30% of the population to download the app.
Here, the dots that have a turquoise circle around them are contacts who have downloaded one of these bluetooth apps. Unfortunately, Bob didn’t, so all of this is worthless in this situation. This is the case 70% of the time if the penetration of these apps is 30%.
Ok, now let’s assume that Bob does in fact have the app installed. No only that, but Bob is very diligent and has it all set up and bluetooth enabled all the time.
In this case, the contact tracer can add 8 of Bob’s contacts — around 15% of the contacts we need. Why so little? Because, for starters, only 30% of Bob’s contacts have the app. Maybe a bit more: Since Bob has the app, it means he’s aware of the need to use the app, and his friends are more likely to be like him. So let’s assume that 40% of his contacts downloaded the app. But many of them never opened it, or never set it up, or did it, but their bluetooth wasn’t enabled when they came across each other.
So 70% of the time we have nothing because Bob doesn’t have the app. Even if he downloaded it, odds are he didn’t open it, or set it up, or have bluetooth enabled. Let’s imagine that only 50% of those downloading it use it as intended. That means 85% of the time, contact tracers stumble upon people who don’t have an app that has any relevant information.
For the rest, around 15% of all infected, only 15% of their contacts have the app properly functioning, for a total overall of around 2% contacts traced.
Remember, this compares to 70%-90% of contacts we need to trace to move from the Hammer to the Dance.
But that’s not all! The way the current apps are set up, people need to self-report their symptoms (which a large share of people won’t do) and then decide actively to send that data to the government.
Many good citizens will do it, but many will not: If they hand off the data to investigators, the likely consequence is that all their family and friends will have to be tested, and many quarantined. If your husband or your friend risks losing their job because they have to stay home for two more weeks, would you hand off this data?
So you might end up with half the amount of contacts traced.
Nobody knows how many people would do each one of these actions, but after working for over 10 years on adoption of tech products, my educated guess on orders of magnitude is the following:
You can play with this simple model here
I might have been optimistic and the share of contacts handed off to contact tracers might be only 0.1%. Or maybe I’ve been pessimistic and it’s 5%. Or even 10%. But with the current approach, it will never be anywhere close to the 70%-90% we want. Every bit counts, but this bit is an awfully small bit.
So what can we do to change this? First, imagine that Apple and Google created an update to the operating system — which they’re working on — but instead of having to download the app, as soon as you update the OS, the app is running in the background, optimized to catch contacts. In such a situation, it’s likely that ~50% of people will update their OS. That is the normal rate within a month.
Let’s assume that, with such an app, Bob still needs to actively tell the app that he’s infected to send his contacts to the authorities. Let’s still assume only 50% do it.
We’re still only at around 10% of contacts! Better than nothing, but it’s still not substantial. Can we do better? Yes.
Let’s assume now that the download of the operating system is automatic. Users might decide to opt out of it, but Apple and Google very heavily insist, every day, for you to update the OS.
Let’s also assume that, since Bob has a notifiable disease, he doesn’t get to choose to upload his list of contacts when he tests positive. It’s uploaded for him.
There is a lot of research that supports the massive difference between an opt-in and an opt-out.
For organ donation, the difference is between ~15% and ~99%. For contact tracing, most people wouldn’t opt out either. And if they do, there are plenty of things we could do to push them to opt-in again, such as asking for a new confirmation every few hours, or asking them to navigate to settings every few hours to confirm the opt-out. Every country might not achieve 99% penetration with an opt-out because of politics, but if we want these apps to be useful, this is the only way.
The point that I am trying to make here is that we need a very, very high penetration of these apps for them to matter, and every decision that users make will drop that significantly. But if we achieve it, the prize is amazing.
Immediately after somebody is known to be sick, authorities could have a list of all the relevant contacts (plus many false positives). The interview with Bob would be a breeze, and all contacts can immediately be called.
And it’s not even that hard to make this happen. Remember the announcement I mentioned before from Apple and Google? What these companies are saying is that they’re first enabling developers to make bluetooth apps that can easily interact with each other. But then they will build these features into their core operating systems. They are planning on making it opt-in, but this could probably be easy to convert into an opt-out, or even forced, if the need is clear enough and governments strongly demand it.
Remember, the point of all this is to keep us above the crucial threshold where contact tracing works well enough to allow the economy to re-open — to shift from the Hammer to the Dance. If opt-outs went from 20% to 5%, a high-enough number of contacts could be traced and sent to the authorities for this to matter.
Let me reiterate that all of the numbers used in this section are illustrative, not real. They illustrate the point that the most important success factor for any contact tracing technology will be adoption.
QR Codes as an Alternative to Bluetooth Apps
Bluetooth apps (or features built into iOS or Android) are not the only way to do this. There are some other interesting alternatives. One of them is through QR codes, like what Zerobase is building.
When you enter a building, you might need to scan a QR code. Scanning it ties you to that place at that time, and everybody else who also tagged around the same time. These codes can be very easily printed and posted anywhere: at the entrance of buildings, of rooms, bus stations, train wagons… The tracking can be done in a way that preserves privacy.
The difference with bluetooth apps is not the technology. Both are pretty great. The difference is the penetration: We could make it mandatory for people to scan QR codes if they want to enter a building. That way, the option to opt out is preserved (don’t enter the building), but the incentive to abide is strong. Something similar could be done with bluetooth apps: If it was mandatory to have one open to enter buildings, penetration might end up high enough.
Note that we still have the problem of self-reporting. We would want a way for the places and contacts to be uploaded to the authorities automatically when Bob is determined to be infected.
That was a lot of information. Let’s summarize all our options, with their pros and cons:
As you can see, I believe apps that require bluetooth opt-in are worthless. QR codes that aren’t enforced are slightly better, because at least Bob can scan it and record where he’s been. But if it’s not mandated, few people and businesses will use it, so few contacts will be recorded.
Manual contact tracing is next. It’s necessary to have manual tracers anyways, so we should do it. But they will trace only part of the contacts, and it will take time. They will also invade the privacy of both the infected and their contacts anyways.
Then we have a series of tech solutions that substantially help contact tracers. Whether through automatic access to Bob’s GPS and credit card data, adding mobile operator-led GPS matches, or opt-out bluetooth contact tracing apps, these provide a substantial amount of information really fast, at a low cost to privacy.
The best options are mandatory QR code or bluetooth apps, They give an immediate dump of contacts, while privacy can be reasonably maintained since the only thing that authorities receive is the person’s information and the list of matches, along with where and when they happened.
For these solutions, authorities wouldn’t need to have more information than this. No need to track every movement for months and store that in a database. Just the matches for the last two weeks, once somebody is proven infected.
Some people might frown upon even this limited amount of privacy reduction. So let’s talk about that.
How Should We Think about Coronavirus and Privacy?
We are scared.
Little by little, all the world we knew around us has disappeared nearly overnight. The jobs, the lives, the freedoms, the friendships we all cherished have been quarantined.
So when we talk about something else taken from us, our privacy, we react. We revolt. We don’t want to lose that too.
Because we understand that the jobs, the friendships, the freedom will come back. But we fear that, if we give up our privacy, we won’t get it back.
We fear 1984.
We want to avoid an AI-driven world where the government knows our every movement, rate us according to our behavior, and soon tell us what to think. We don’t want to be China.
That is not just a theoretical nightmare. The US is still under the Patriot Act, approved 19 years ago on the wake of 9/11.
This fear is good, because it makes us alert. It makes us pay attention. It makes us appreciate the freedoms we have and fight to defend them, because if we lose them today, we might never get them back.
But that fear can’t be irrational. It can’t be all-encompassing. It can’t devolve into panic.
We need to look at the problem coldly, break it down, and rationally decide a course of action.
The first way we break it down is realizing that this is not about everybody’s data, but rather that of two small groups: the infected and their contacts.
The infected already have different privacy rights. Many countries already have legislation to treat them differently. And we want them to. Would we want the infected to be able to not collaborate with authorities to reduce the impact of the epidemic? The only debate here is the level of privacy they should be allowed to keep.
All the proposals here suggest that the only data that needs to be known about the infected is where they’ve been over the last two weeks and with whom. Asking them directly is faulty. Getting that information through GPS, credit card spending patterns, or mandatory bluetooth apps is reliable and immediate, while limiting the exposure to less than police can already find out about any one of us.
As for their contacts, their privacy rights should be slightly higher. We don’t need their credit card statements, or their entire mobility data. We just want to know who they are and the interaction they’ve had with infected people: where, when, and for how long. We only want that information for the last two to three weeks. That information can be gathered through mandatory bluetooth apps, mandatory QR codes, reports from mobile operators, and probably other tools. Governments don’t need to know more than that. Just that.
That suggests a list of limitations to the data that authorities should be able to gather:
- Limits to data gathered: For infected people, we will only gather their whereabouts, who they met, where, and for how long. For their contacts, just that there was a contact, where, and for how long.
- Limit to time: Data will only be accessible for the three previous weeks. All previous data will be deleted.
- Access: Only the Ministry of Health or equivalent regional agency should have access to data collected under legal process from private companies or by investigators in interviews. Who has access to the data within the Ministry of Health (eg, investigators) should be clearly stipulated, carefully monitored by tracking every time an employee accesses a piece of data, and subject to robust auditing.
- Security: All the PII will be protected to match medical standards.
- Clearly defined exit criteria: We need this data only during the epidemic. The definition of “Epidemic” needs to be objective and clearly stated. For example, once more than 70% of the population becomes immune, either through vaccination or herd immunity, the data gathering system will be automatically shut down and the data collected will be destroyed.
- Due process: People must have recourse to the courts if the government has used data in a way that was unintended, or if the conclusions reached by investigators are unfair or inadequate.
- Transparency: All the information collected should be made explicit. It should also made public, extracting all personally identifiable information (PII): things like names or addresses.
Privacy professionals could offer more specifics on how to protect location history data. For example, we could have all the contact tracing operation run by a corporation or a non-profit — or a set of them. They could simply communicate to the authorities who should be isolated and who should be quarantined for enforcement. Maybe people could not opt out of sharing the information, but they can choose to whom they give it.
The second way we can look at this problem is through the data we don’t want the government to have. Most people are likely fine sharing with the government matches with infected people they’ve had over the last two weeks. What they don’t want is the government to know all their movements.
But it already can.
Not just because it already has vast amounts of data, in a country like the US from the IRS, the DHS, the FBI, and other bodies. Also, because a lot of this information is already available from private companies.
As the New York Times reported, dozens — if not hundreds — of companies gather and sell much more data than what is required here. Companies like Google, Apple, Waze, Uber, IBM, Kiip, TheScore, Facebook and dozens more know where you are and where you go all the time, and many sell that information.
Companies already share that they know 5,000 data points per user. That might be more than you know about yourself. That information is sold anonymized sometimes, but it can be de-anonymized.
So we are debating to share with companies, NGOs or governments a small amount of information that is much less than what can already be bought online — and is much more concerning than sharing if you met Bob for lunch last week.
The third way we can break down this problem is through buying ourselves options. Some of the systems described here might still be polemic, but we might want to build them now nonetheless, without approving them yet. If we wait for months to resolve the debate, and suddenly a new outbreak happens, we might need to decide between trillions of dollars in economy closures or flipping up a switch and using this technology. But we can only do that if the technology is available. If we want to use, for example, bluetooth applications mandated for all, we need to build that now to have the option in a few months.
Finally, we should put privacy in context of the other rights we’ve lost. We’ve lost our health. We’ve lost our economy. We have lost our freedom. If we can get them back with a little bit of privacy, are we not going to consider it? The $2 trillion package approved in the US is equivalent to $10,000 per adult. Are you really sure you’d rather pay $10,000 than give the government a bit of information you already give to FourSquare?
So to summarize, we just want to share a little bit of data, that can be heavily limited, that is much less than what is already publicly available — or available to the government — , about very few people. All so that we can get back our health, our economy, our freedom, and our lives.
Humans aren’t meant to be isolated. We’re meant to dance.
This section draws heavily on ideas and sources from @Genevieve Gee’s research on Contact Tracing.
If you want to receive the next installments of the article, sign up for the newsletter.
If you want to translate this article, do it on a Medium post and leave me a private note here with your link.
Translations
Spanish
German
Italian
Vietnamese
Ukrainian
Russian
Portuguese
Japanese (alternative, alternative outside of Medium)
Dutch
Farsi
Bulgarian (only testing)
Thai
Macedonian
This is Part 3 of our Article, Coronavirus: Learning How to Dance. In Part 1, we discuss best practices from Taiwan, Singapore, China and South Korea. In Part 2, we discuss masks. In Part 4, we will talk about Isolations and Quarantines. In Part 5, we talk about Travel Bans, Limits to Social Gatherings, and Economic Closures. In Part 6, we will put all of it together. We will give specific recommendations on each, including a warning: Most countries are not approaching the Dance well. If they continue their current path, they will end up like Singapore.
This has been a massive team effort with the help of dozens of people who have provided research, sources, arguments, feedback on wording, challenged my arguments and assumptions, and disagreed with me. Special thanks to Genevieve Gee, Matt Bell, Berin Szoka, Carl Juneau, Jorge Peñalva, Christina Mueller, Barthold Albrecht, Elena Baillie, Pierre Djian, Yasemin Denari, Shishir Mehrotra, Eric Ries, Kunal Rambhia, Jeffrey Ladish, Claire Marshall, Manik Gupta, Brian McClendon, Donatus Albrecht, the Test and Trace team, and many more. This would have been impossible without all of you.
If you want to know the latest about Testing and Contact Tracing in the US, go to Test And Trace.
